Anterior Knee Pain
ANTERIOR KNEE PAIN CAN BE CAUSED BY A NUMBER OF FACTORS SUCH AS THE FOLLOWING:
• Muscle weakness around the knee
• Overload in the knee due to training demands/repetitive loading
• Muscular imbalances elsewhere in the lower limb causing compensatory load to the knee
• Conditions such as knee bursitis, knee OA, Osgood Schlatter’s (in adolescents)
• Ligament/meniscal injury
While there are several causes for knee pain, the rehab framework I use for each is very similar. For this case study, we will take anterior knee pain without a traumatic history i.e. knee pain that has developed without a significant injury event/mechanism in both the active and inactive individual.
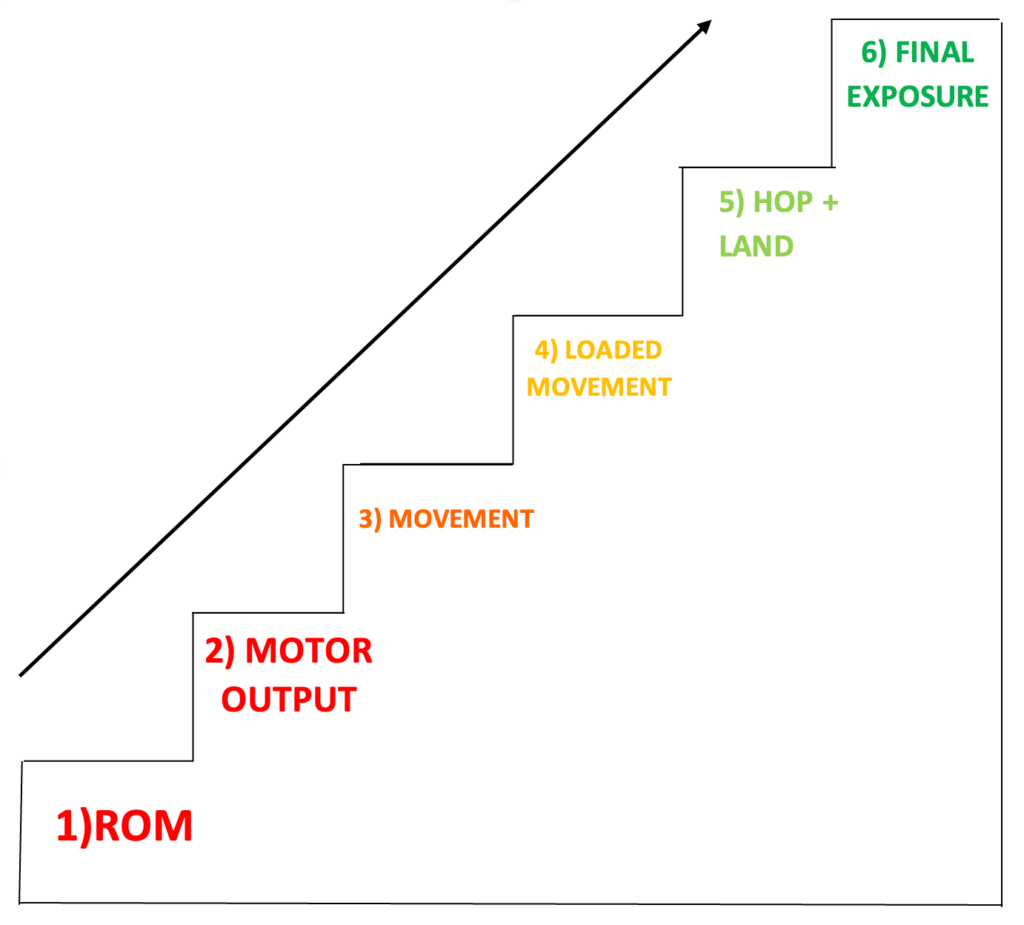
The diagram to the right is the framework I had picked up on and which I use for the rehabilitation of any injury. This is also helpful as a tool to explain to clients why we are doing specific movements and exercises using a chronological and specific approach. The subjective and objective assessment will directly correlate to what the main focuses of rehabilitation should be. For this case study, I will break down each step as well as showing the types of exercises that can be done relevant to that stage.
I would also like to point out that this framework can be utilised with all types of populations, regardless of active/inactivity levels and can be adjusted relative to the patient. In addition, each stage will look different relative to the individual. For example, a strength movement for an athlete may be a squat with load whereas for an individual with reduced mobility it may just be a sit to stand. Therefore, both exercises are deemed as high effort but relative to the individual.
RANGE OF MOTION (ROM)
Range of motion describes the ability to move through range with a joint. In terms of the knee, this relates to knee flexion (bending) and knee extension (straightening).
Problems that can occur with having reduced ROM is that the muscles are restricted in their ability to lengthen and contract due to its muscle length being restricted. Therefore, before any strengthening, restrictions in ROM have to be addressed.
Below are some examples of drills to increase ROM:
MOTOR OUTPUT
Motor output describes the ability for muscles to maintain control/firing over a prolonged period (4-6 seconds) using only 40-50% of their maximum muscle strength/power. The inability to maintain control at this level can cause other structures to overload and compensate further down the rehabilitation steps.
For anterior knee pain, reduced motor output can not only be found with the quadriceps, but also in the hip flexors, adductors/groin muscles, hamstrings, glutes and calves. This can also suggest that the knee pain is a symptom rather than the cause in some cases due to other muscles under working and the quadriceps having to take the extra load resulting in pain/overload.
There is an array of ways to elicit this positive addition and can be adjusted for all types of populations. For example, for an individual with less mobility, seated versions of the exercises can be done. In comparison, with an athlete I would look to still incorporate a high level of activity elsewhere and/or in more athletic positions.
Therefore, exercises using Isometrics are useful to address these issues.
To the right is an example drill to increase Motor Output:
MOVEMENT
Moving into the movement phase includes implementing basic lower limb movement patterns which can be summarised as the following: squat, lunge and hinge.
It is crucial to master these movements to rebuild control, stability and foundational strength before progressing to the next phase. I would usually focus on one plane of movement (for example forward) before progressing to exposure in different planes (sideways) as well as going from double leg to single leg to increase difficulty.
In a non-athlete/inactive population, this could simply be a sit to stand with its progression to bias one leg.
Below are a couple of examples of exercise progressions for the lunge movement pattern:
LOADED MOVEMENT
Once the foundational movement patterns are mastered, we simply add load to these movements via resistance bands, free weights etc This would be targeting the strength aspect of the rehabilitation.
At this point, due to the intensity of exercises increasing, the frequency of the exercises with reduce to avoid excessiveness soreness and promote recovery between sessions. An example of 2-3 sessions per week would be programmed at this point.
For athletes this may be a heavy loaded back squat with a barbell but for non-athletes, this may simply be a tempo squat or using external load such as a backpack.
Below are some examples of loaded movements:
HOP AND LAND
After building strength during the previous phases, we then move to implement more power-based/plyometric type movements to take advantage of that strength gained previously. This allows people to retrain their muscles and joints to absorb high-impact forces as well as producing high forces. These can be progressed from double leg to single leg as well as combining planes of movement. This can also be achieved by using lighter loads and moving at speeds.
This is important to develop for sports such as tennis, football, running etc all of these require high-impact forces to be taken by the knee as well as changes in direction.
In comparison, for a non-active population with reduced mobility, this may simply be stepping off a step to emulate everyday activities with stairs to retrain taking impact. This still targets the power aspect of the rehabilitation but again is relative to the individual.
Below are some examples of power-based drills:
FINAL EXPOSURE
This is the end stage of the rehabilitation which includes a phased return to sport-specific training with increased intensity over time to allow people to adapt and rebuild confidence again.
An example of using football would be starting with cone drills and increasing pace, then implementing a change of direction component. Once comfortable, then a ball would be added to the drills to increase the difficulty as well as later on adding another player to the drills to mimic game scenarios. Thereafter, increasing intensity and unpredictability as the last progression then finally full contact in training and return to play.
For a non-athlete individual, this may just be a return to a walking programme with simply progressing distance and frequency covered back to their previous baseline.
WE HOPE YOU’VE ENJOYED THESE TIPS FROM OUR PHYSIO ADAM
After graduating with a BSc degree in Physiotherapy, Adam’s clinical experiences so far have seen him manage a range of post-operative cases, as well as the regular assessment and rehabilitation of many musculoskeletal problems.
Adam works to empower patients with their own rehabilitation journeys back to their desired goals by utilising an exercise and holistic driven approach.
If you’d like to book an appointment with Adam you can do so here or give us a call on 0800 731 2738.